Shift Scheduler Blog
How We Helped a Ward Sister Save 3 Days on Monthly Nurse Rostering

Planning nurse shifts is not just filling names into a calendar.
In a hospital ward with 24/7 operation, every rota has to balance staffing needs, qualifications, leave requests, personal preferences, fairness, rest periods and last-minute changes.
In this anonymised case study, we show how Shift Scheduler helped a ward nurse plan a monthly rota for 25 nurses and save approximately 3 days of work.
The ward operated continuously, with day shifts and night shifts. Across the schedule, there were 8 shift slots per day, over a 28-day planning period. Some shifts also required a specific qualification mix — in the Slovak workspace, this was marked as ARIP/VŠEO. In a UK context, this can be understood roughly as a combination of critical care / intensive care nursing capability and Registered Adult Nurse / Registered Nurse coverage. The Nursing and Midwifery Council lists Adult Nurse and General Nurse registration codes, while UK critical care nursing programmes are commonly aimed at qualified nurses working in intensive care or critical care settings.
What Actually Took 3 Days
The biggest problem was not the calendar itself.
The problem was everything that had to happen before the ward nurse could even start building the rota.
Leave requests and personal preferences were arriving through different channels. Some nurses sent emails. Some gave their requests verbally. Others handed in notes on paper.
That created several problems.
First, the ward nurse had to collect all the information manually. Then she had to consolidate it into one place. Then she had to check whether two nurses had requested the same day off. If they had, she had to find out who requested it first.
This alone took a serious amount of time.
The issue was not only "who wants which day off". The issue was also priority. When several people asked for the same dates, the ward nurse needed a fair way to decide whose request came first.
After that, she still had to build the actual schedule.
And after the first draft was ready, the second wave of work started: complaints, fairness checks and revisions.
Nurses regularly questioned whether the rota was fair. For example:
- Why do I have more night shifts than others?
- Why do I have fewer day shifts?
- Why am I working this weekend again?
- Why was my leave request not respected?
- Why am I scheduled after a difficult run of shifts?
- Why is someone else getting a better pattern?
Each complaint required checking the rota again, explaining decisions, changing assignments and making sure that one fix did not create another conflict somewhere else.
That is where the 3 days went.
Not into one single task, but into a chain of manual work: collecting requests, comparing priorities, drafting the rota, checking fairness, communicating changes and revising the schedule again.
The Scale of the Problem
In this case, the ward nurse had:
- 25 nurses
- 28 days
- 8 shift slots per day
- day and night coverage
- leave requests
- individual preferences
- qualification requirements
- rest rules
- fairness expectations
That means she had to fill:
- 8 shift slots × 28 days = 224 shift assignments
If we simplify the problem and say that each shift slot could theoretically be assigned to any of the 25 nurses, the number of possible combinations is in millions.
The important point is this: a human planner is not choosing between 10 or 20 options. She is navigating an astronomical number of possible combinations, while also trying to satisfy rules that constantly interact with each other.
This is why shift scheduling is not just an administrative task. It is a constraint optimisation problem.
How Shift Scheduler Changed the Process
The biggest improvement was not only automatic rota generation.
The real improvement was that the whole planning process became structured.
Instead of collecting leave requests from emails, paper notes and verbal messages, each nurse could submit leave or availability through her own account, from a phone or computer.
The ward nurse then had all requests in one place.
She could see:
- who requested leave,
- which dates were requested,
- when the request was submitted,
- which requests came first,
- which requests were still pending,
- which requests had already been approved or rejected.
This removed the first major manual task: consolidating requests.
It also removed a major source of disputes. When priority matters, the system can show the order in which requests were submitted. The ward nurse no longer has to search through emails, paper notes or memory.
The Rules We Modelled
The second major improvement was that the ward's planning rules were entered directly into the system.
Some rules were hard constraints that should not be broken. Others were preferences that the system should follow where possible.
Below is an anonymised version of the rules used in the workspace. Real names were replaced with Nurse 1, Nurse 2, Nurse 3 and so on.
General rules
- Each person can have at most one shift per day.
- No person should have more than two day shifts in a row.
- After a night shift, there must be two days off.
- Selected shifts requiring ARIP/VŠEO coverage can only be assigned to nurses with the relevant qualification tag.
- In a UK context, this is comparable to requiring the right mix of Registered Nurse / Registered Adult Nurse coverage and critical care or intensive care nursing capability.
Individual nurse rules
- Nurse 1 can work only night shifts in odd weeks and only day shifts in even weeks.
- Nurse 2 cannot work on Mondays or Fridays, and cannot work night shifts on Thursdays or Sundays.
- Nurse 3 can work night shifts anytime, day shifts anytime during weekends, day shifts only on Mondays and Wednesdays in odd weeks, and day shifts only on Tuesdays and Thursdays in even weeks.
- Nurse 4 cannot work day shifts on Mondays or Thursdays.
- Nurse 5 cannot work night shifts on Mondays and cannot work either day or night shifts on Tuesdays.
- Where possible, the preferred pattern is: day shift, then night shift, then at least two days without a shift.
- A full-time workload is 38.75 hours per week. For part-time nurses, the planned workload is reduced proportionally.
- Nurse 6, Nurse 7, Nurse 8 and Nurse 9 should not work together.
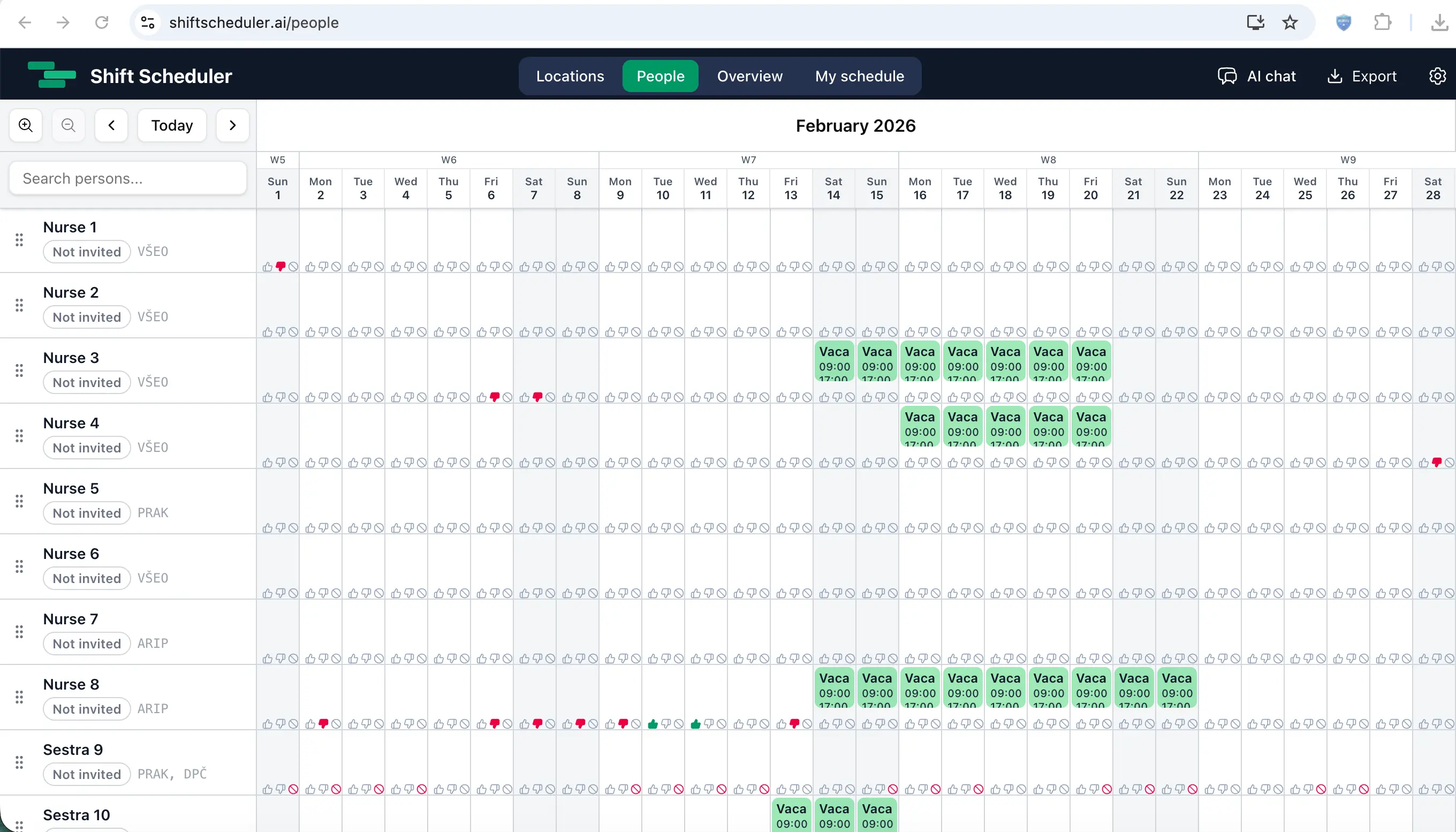
This is how the workspace looked after all preferences and vacation requests had been collected from the team — before the rota was generated.
This is exactly the kind of rule set that becomes painful in a spreadsheet.
One rule is manageable. Twelve rules are still manageable if they are independent. But when these rules interact with 25 people, 224 shift slots, holidays, qualifications and fairness expectations, manual planning becomes fragile.
Changing one shift can break three other rules.
Why Fairness Became Easier to Defend
Fairness was one of the most important parts of the case.
Before Shift Scheduler, fairness complaints created a lot of extra work. A nurse could say she had too many night shifts, too few day shifts, too many weekends, or a worse pattern than someone else.
The ward nurse then had to check the schedule manually and explain the decision.
With a structured system, fairness becomes easier to measure.
Instead of relying only on subjective impressions, the system can track the number of day shifts, night shifts, weekends, total hours and workload distribution.
That does not mean every nurse will always get exactly what she wants. In a 24/7 environment, that is not realistic.
But it means the final schedule is easier to explain.
The discussion changes from:
"I think this rota is unfair."
to:
"Here is how many day shifts, night shifts and total hours were assigned. Here are the constraints that caused this result."
That matters.
A rota does not only need to be operationally correct. It also needs to be credible to the team.
What the Ward Sister Still Controlled
AI did not replace the ward nurse.
That is the wrong way to think about this kind of automation.
The ward nurse still controlled the important decisions:
- which rules are strict,
- which rules are preferences,
- which leave requests can be approved,
- which exceptions are acceptable,
- when human judgement should override the system,
- whether the final rota is operationally safe.
Shift Scheduler handled the computational burden.
It checked combinations, applied constraints, respected leave, considered qualifications and helped distribute work more fairly.
The ward nurse moved from manually building the rota from scratch to reviewing and adjusting a structured proposal.
That is a better use of her time.
The Result
For this ward, Shift Scheduler helped save approximately 3 days of work on one monthly rota.
The ward nurse no longer had to start from a blank spreadsheet. She had a structured workspace with nurses, qualifications, leave requests, preferences and rules already in one place.
The system could then generate a rota that respected the core constraints and gave her a much better starting point.
The final decision still stayed with the ward nurse. But she no longer had to spend days collecting requests, checking conflicts and defending every change manually.
Why This Matters
Healthcare shift planning is often treated as back-office administration.
It is not.
Bad scheduling affects staff fatigue, fairness, morale, qualification coverage and operational stability.
For a 24/7 ward, the rota is part of the operating system of the department.
When planning is done manually, too much depends on one person's memory, patience and ability to keep hundreds of constraints in mind at the same time.
AI shift scheduling does not remove the need for human judgement. It gives the person responsible for the rota a better tool.
In this case, that meant one ward nurse getting back approximately 3 days per month.
Not by cutting corners.
By replacing fragmented, manual and repetitive planning work with a structured, transparent and algorithmically checked workflow.